

In 1905, Sigmund Freud proposed a theory: young girls experience “clitoral” orgasms. Mature women graduate to “vaginal” orgasms. Failure to make this transition indicated psychological immaturity — an inability to accept one’s adult sexual role.
This theory had zero anatomical evidence. Freud had never dissected a clitoris. He’d never studied female pelvic innervation. He simply decided, from his armchair in Vienna, what female pleasure should look like, and then pathologized everyone who didn’t fit.
More than a century later, I still receive messages every week from women asking some version of: “I can only orgasm from clitoral stimulation. Is something wrong with me?”
Let me be as clear as humanly possible: nothing is wrong with you. Freud was wrong. And the anatomy that proves it has been publicly available for decades — we just haven’t done a good enough job making sure every woman knows about it.
This article explains what the science actually says about clitoral and G-spot orgasms, why they’re not competing categories, and practical techniques for experiencing both. No psychoanalysis. No judgment. Just anatomy, evidence, and usable information.
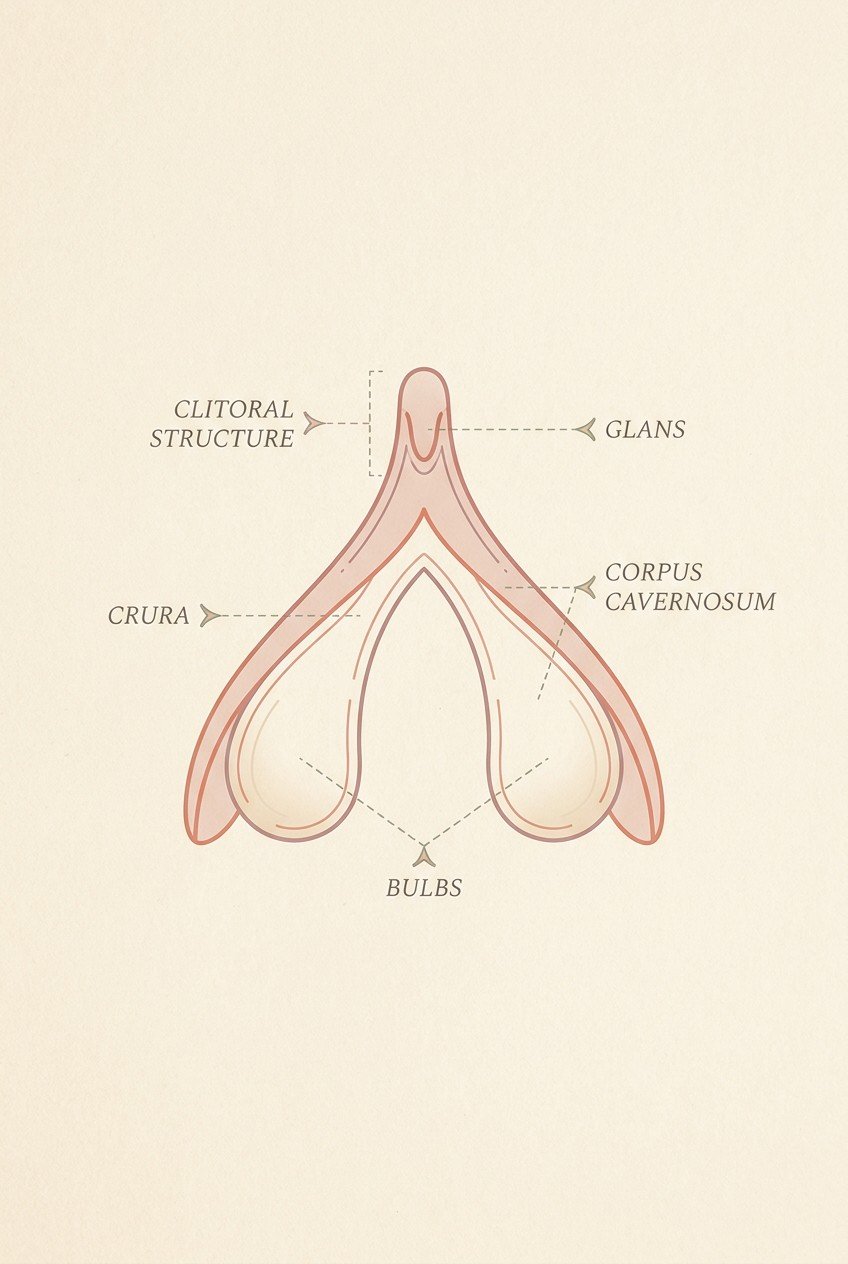
Most people picture the clitoris as a small external nub — the glans, visible at the top of the vulva where the inner labia meet. That’s the part you can see. It’s also the smallest part of the entire structure.
The full clitoris is a wishbone-shaped internal organ, roughly 9–11 centimeters in total length, with branches that extend down both sides of the vulva and wrap around the vaginal canal. It’s composed of erectile tissue — the same type of tissue that makes up the penis. It engorges with blood during arousal. It has approximately 8,000 nerve endings in the glans alone, making it the most densely innervated structure in the human body.
Here’s the part that changes everything: the internal branches of the clitoris — called the crura and the bulbs — sit directly behind the front wall of the vagina. When you stimulate the so-called “G-spot” through the vaginal wall, you are not stimulating a separate organ. You are stimulating the internal portions of the clitoris from the other side.
The G-spot is not a gland. It’s not a magical button. It is the area where the internal clitoral network comes closest to the vaginal wall — roughly 2–3 inches inside, on the front wall, toward the belly button. The tissue there is spongy and ridged because it’s the back of the clitoral bulbs and the urethral sponge (the female equivalent of the prostate).
This is why almost every woman who experiences “G-spot orgasms” also requires external clitoral stimulation — or some form of simultaneous stimulation that activates the entire network. The idea of a “purely vaginal” orgasm isolated from the clitoris is anatomically misleading. All orgasms involve the clitoris. The difference is how you stimulate it.
Think of it like listening to music. You can hear a song through speakers placed directly in front of you (external clitoral stimulation). You can also feel the bass through the floorboards, vibrating up through your body (internal G-spot stimulation). The song is the same. The pathway is different. One isn’t more “mature” than the other. The floor doesn’t make you a better listener than the speakers.
The implication: you don’t need to graduate from one type of orgasm to another. Your body isn’t failing a test Freud wrote in 1905. If you experience clitoral orgasms and not G-spot orgasms, your clitoris works perfectly. You may simply not have found the right angle, level of arousal, or technique for internal stimulation — or your internal clitoral branches may simply be less sensitive than your external glans. Both are normal variations. Neither is a defect.
Science describes nerve pathways. Experience describes sensation. Both matter. Here’s what women consistently report across studies and clinical settings.
Location: Precise and focused. You know exactly where it’s coming from — the external glans and the area immediately around it. The sensation is sharp, acute, and localizable to a specific point.
Quality: Intense, often described as a peak or spike. Builds rapidly. Peaks sharply. For many women, the peak is higher than internal orgasms — more concentrated, more electric. But it often fades quickly after the peak. The comedown is relatively fast.
How it feels during: A rising tension focused entirely in the external area. As it builds, the sensation can feel almost too intense — many women need to reduce or redirect stimulation at the peak. Pulsing contractions, usually 5–8 rhythmic waves, centered in the pelvic floor.
What makes it easier: Direct, consistent stimulation to the clitoral glans. Vibration is highly effective. Most women can reach clitoral orgasm with a vibrator within 5–15 minutes.
What can make it harder: Overstimulation. Starting at too high an intensity. Insufficient lubrication creating friction that feels sharp rather than smooth. Mental distraction — clitoral orgasms require sustained focus for many women.
Location: Diffuse and deep. Most women can’t point to exactly where it’s coming from — it feels like a wave spreading through the pelvis, lower abdomen, and sometimes down the inner thighs. The sensation is full rather than pointed.
Quality: Slower build, longer peak, longer comedown. Often described as a wave rather than a spike. The peak may feel less acute than a clitoral orgasm — less of a sharp explosion, more of a sustained flood. But the sensation lasts longer, and the afterglow is deeper. Some women report feeling emotionally moved afterward in a way that clitoral orgasms don’t produce — likely because the internal stimulation activates different autonomic nerve pathways.
How it feels during: A growing sense of fullness and pressure that transitions into rhythmic internal contractions. These contractions are often described as “pulling” or “gripping” rather than the pulsing of a clitoral orgasm. The sensation spreads rather than concentrating.
What makes it easier: High arousal BEFORE stimulation. The G-spot becomes prominent only when the internal clitoral tissue is engorged — which requires significant arousal first. Women who try G-spot stimulation from a cold start often feel nothing because the tissue hasn’t swelled yet. This is the single most important practical insight in this entire article.
What can make it harder: Insufficient arousal. The wrong angle — the G-spot is on the front wall, and stimulation needs to curve upward. Mental pressure — trying to “achieve” a G-spot orgasm creates the kind of performance anxiety that actively prevents one.
There is a persistent cultural narrative that G-spot orgasms are “deeper,” “more real,” or “more mature” than clitoral orgasms. This is Freud’s ghost, still haunting bedrooms 120 years later.
There is no hierarchy of orgasm types. A clitoral orgasm is not a “starter” orgasm. A G-spot orgasm is not a “real” orgasm. They are different sensory experiences facilitated by different types of stimulation of the same organ system. Preferring one over the other is like preferring chocolate ice cream over vanilla. It’s a preference. Not a developmental achievement.
Not because you’re broken. Because of variables you can actually influence.
Just as some people have more sensitive fingertips than others, the density of nerve endings in the internal clitoral tissue varies from woman to woman. This is genetic, not behavioral. If your G-spot area is less sensitive, you may need more pressure, more arousal, more time, or a combination of all three. It doesn’t mean stimulation won’t work — it means the threshold is higher.
Conversely, some women have exceptionally sensitive internal clitoral tissue and can orgasm from vaginal penetration alone, even without targeted G-spot stimulation. This is the minority, not the norm. Pornography has convinced a generation of people that it’s the default. It isn’t. Studies consistently find that only 18–25% of women report being able to orgasm from vaginal penetration alone.
I said this in the previous section, and I’m repeating it because it’s the most actionable piece of information in this article: the G-spot tissue must be engorged to be sensitive.
When you’re not aroused, the internal clitoral bulbs are deflated. The vaginal wall is relatively smooth and insensitive. Pushing on it feels like pushing on any other internal surface — neutral, maybe slightly uncomfortable.
When you’re highly aroused, those same bulbs fill with blood. They swell. They press against the vaginal wall. The spongy, ridged texture becomes palpable. Now pressing on it feels like pressing on erectile tissue — because that’s exactly what it is.
The practical implication: Don’t start with G-spot stimulation. Start with whatever reliably arouses you. External clitoral stimulation. Oral sex. Whatever your body responds to. Once you’re fully aroused — and I mean fully — then introduce G-spot stimulation. The difference is night and day.
The G-spot is on the front wall of the vagina. In certain positions, gravity and internal organ placement push it closer to the surface, making it much easier to reach.
Best positions for G-spot access:
Position to avoid during learning: Lying completely flat with legs straight. The vaginal canal elongates, and the front wall angles away. G-spot access becomes minimal.
This is the “blended” approach, and it’s the most reliable path to G-spot orgasm for most women.
The technique: provide steady G-spot pressure with a curved toy or fingers inside, while simultaneously stimulating the clitoris externally with a bullet vibrator, your other hand, or oral sex. The external stimulation keeps your arousal high. The internal stimulation has time to build slowly, without the pressure of being the sole source of sensation. Over several minutes, the internal sensation often “catches up” — the G-spot tissue becomes sensitized enough that the internal pressure starts competing with the external vibration, then briefly overtakes it. That’s the blended orgasm.
This is also why rabbit vibrators have dominated the market for 30 years. They do the simultaneous part automatically.
Yes. It’s called a blended orgasm, and for many women, it’s the most intense type.
A blended orgasm occurs when external clitoral stimulation and internal G-spot stimulation peak simultaneously. The neural signals from both pathways converge in the spinal cord and amplify each other. The result is typically described as deeper, longer, and more physically overwhelming than either type alone.
How to work toward one:
Some women also experience sequential orgasms: a clitoral orgasm followed, 30–90 seconds later, by a G-spot orgasm triggered by continued internal stimulation. The refractory period between orgasms is typically much shorter for women than for men, making multiple orgasms physiologically achievable for most women — although not all women want them, and not all women are multi-orgasmic. Again: all variations are normal.
Different orgasm types benefit from different toy designs. Here’s the practical match.
| Orgasm Type | Best Toy Type | Why |
|---|---|---|
| Clitoral | Bullet vibrator, wand, suction toy | Concentrated external stimulation on a small area. Adjustable intensity. |
| G-Spot | Curved G-spot vibrator, glass or metal G-spot wand | The upward curve presses into the front wall. Firmer materials transmit pressure better than soft silicone. |
| Blended | Rabbit vibrator | Simultaneous external ears + internal curved shaft. Dual motors allow independent intensity control. |
| Clitoral → G-Spot upgrade | Bullet + G-spot toy used as a pair | Use the bullet externally first, then introduce the G-spot toy while keeping the bullet in place. |
| Beginner (not sure) | Bullet vibrator + small curved silicone dildo | Low cost, low pressure. Try separately, then together. Learn what your body responds to before investing in specialty toys. |
One important product note: For G-spot stimulation specifically, firmer materials (glass, metal, hard ABS plastic, firm silicone) often work better than soft silicone. Why? Because the G-spot responds to pressure, not friction. A soft toy absorbs some of the pressure you’re applying. A firm toy transmits it directly. This is one of the few cases where “softer” is not better. For a complete breakdown of which materials are safe for which types of stimulation, see our body-safe materials guide.
No. Some women discover G-spot orgasms in their 40s. Some never do. Some simply prefer clitoral stimulation and have no interest in exploring internal stimulation. All of these are complete, valid sexual experiences. The presence or absence of G-spot orgasms does not measure your sexual maturity, health, or worth.
Probably not. G-spot orgasm requires a specific angle, sustained pressure, high arousal, and most importantly — your own familiarity with the sensation. Most women who achieve G-spot orgasms with partners learned to find them alone first. Once you know the angle and the pressure that work for you, you can guide a partner to replicate them. Expecting a partner to discover your G-spot by trial and error is like expecting someone to find a specific book in a library without knowing the title, the section, or the author.
Use it, but use less than you would for external stimulation. G-spot stimulation relies on pressure, not friction. Too much lubricant can reduce the pressure sensation by creating a slick surface that slides over the G-spot rather than pressing into it. A small amount — enough to make insertion comfortable — is all you need. Reapply to the vaginal opening if needed, not the G-spot area. For a full guide to choosing the right lubricant for different types of play, read our complete lube guide.
No. The G-spot area is nerve tissue and erectile tissue, not a muscle that can be fatigued or a surface that can be callused. It does not become “numb” from regular stimulation. If stimulation feels less intense than usual, the issue is almost certainly insufficient arousal — your internal tissue isn’t engorged. Take a longer warm-up period before trying again.
Then you are one of millions of women whose G-spot area is less sensitive, and that is a neutral characteristic of your anatomy — like having blue eyes or curly hair. It doesn’t mean your sex life is incomplete. It doesn’t mean you’re missing out on some universal female experience. It means your body responds to one pathway and not the other. Honor that. Work with it. Don’t fight it because a man in 1905 decided it meant you were immature.
Here’s what I want you to take from this article, condensed into the fewest possible words:
The G-spot is part of your clitoris. Clitoral orgasms and G-spot orgasms are different pathways to the same destination — not competing achievements. One is not better than the other. You are not broken, immature, or incomplete if you’ve only experienced one type. Freud was wrong. The anatomy proving it has been available for decades. Your pleasure belongs to you, not to a psychological theory from 1905.
If you want to explore G-spot orgasms, start with high arousal. Use a firm, curved toy. Experiment with position. Combine external and internal stimulation. Give yourself time and remove performance pressure. If it happens, wonderful. If it doesn’t, wonderful. Neither outcome defines your sexuality.
You don’t need to graduate from anything. You’re already here.
Ready to explore? Browse our vibrator collection — including G-spot toys, rabbit vibrators, and bullets designed for every type of stimulation. Body-safe. Honest reviews. No psychoanalysis.
About the Author:
Dr. Yuki Tanaka is a sexual health educator and pleasure researcher at AmorSerere. With a PhD in human sexuality and 8 years of clinical education experience, Dr. Tanaka specializes in translating peer-reviewed sexual health research into practical, stigma-free guidance. Her mission: replace century-old myths with actual anatomy, one article at a time.
Last Updated: July 9, 2026

Clinical sex educator with 10+ years experience. Specializes in body-safe materials and sexual wellness education.